A 62 year old gentleman is 6 days post cardiac bypass surgery. The ICU has had difficulty weaning the patient from the ventilator.
Over the past 24 hours, the patient's ventilator requirements have increased. There have also been an increase in endotracheal secretions.
You perform a bedside ultrasound, which reveals this image:
This is an example of consolidation seen on ultrasound secondary to a ventilator-associated pneumonia. Non-translobar consolidation is confirmed by the "shred sign", which is seen as the irregular line at the bottom of the screen. This irregular line marks the boundary between the consolidated and non-consolidated lung.
It is important to differentiate atelectasis from pneumonia when consolidation is present on ultrasound. The dynamic air bronchograms, as seen above, are more suggestive of a pneumonia. In the image above, clear, anechoic airways are visualized, and these airways change dynamically during inspiration and expiration.
For more information on signs of consolidation and dynamic air bronchograms, check out Dr. Lichtenstein's videos below.
This app provides information on interpretation of ultrasound images in 6 systems:
In each system, a labelled image with normal values for ultrasonography interpretation is presented. See the aortic root example below:
This App provides a quick reference to look up the relative position of structures in various ultrasound views as well as the normal reference ranges for these structures. However, this App does not provide information on probe positioning or on capturing these images. This App serves as a good resource for quick identification and interpretation of various structures in the systems listed above.
Another good feature of this App is the "Links" Section on the home page, which provides links to Emergency and Intensive Care Ultrasound resources, online lectures, image archives and core articles. Some of the links don't work, but most of them do work and provide great background information on point of care ultrasound.
Overall, this App serves both as a quick reference guide for point-of-care ultrasound interpretation as well as a source of information for those with background knowledge in point-of-care ultrasound.
These two videos demonstrate the ultrasound techniques for femoral artery and vein catheter insertions.
First, the femoral artery catheter insertion:
Second, the femoral vein catheter insertion:
These are both very similar, since you will be locating both the femoral artery and vein when you perform either procedure.
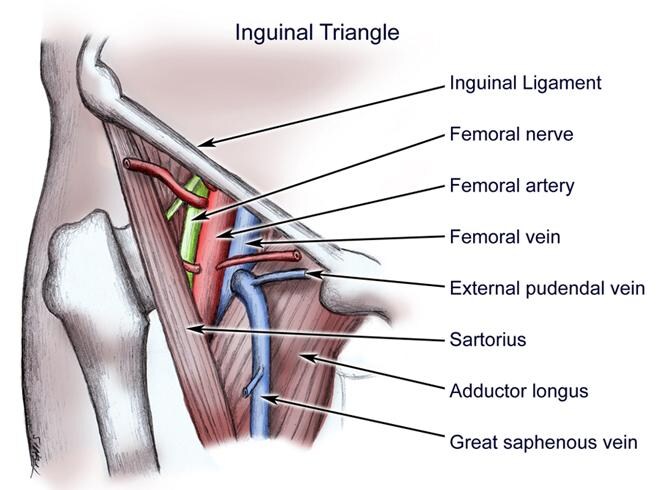
Localization of both of these structures is key when performing these procedures. It is important to remember the anatomy of the femoral region. The femoral artery runs laterally to the femoral vein and medially to the femoral nerve as in the figure below.
However, anatomical variants do exist, so this is not always the case. To further help with localization of your chosen vessel, remember that that veins are compressible on ultrasound, while arteries are not.
A 63-year old lady was admitted to the coronary care unit post cardiac arrest with return of spontaneous circulation. She was intubated for a decreased level of consciousness following resuscitation and was placed on a hypothermia protocol. You are called to assess her for low blood pressure and increasing oxygen requirements.
On exam, her blood pressure is 100/60 with a pulse of 90. Temperature is at target for the hypothermia protocol. Oxygen saturations are 90% with an Fi02 of 0.8 and a PEEP of 10 cm H20. Her JVP is difficult to appreciate. Heart sounds are rapid, with no additional heart sounds or murmurs appreciated on initial assessment. There are crackles on lung auscultation.
You quickly review the chart, and noticed that this patient was given a 500 mL bolus earlier this afternoon for hypotension and decreased urine output. Her urine output has been minimal (30 mL total) since the bolus 4 hours ago. Also, the PEEP has been increased from 8 to 10 cm H20, and the Fi02 was progressively increased from 0.6 to 0.8.
You've ordered an initial chest X-ray, ECG and bloodwork. While waiting for these tests to be performed, you perform a quick bedside lung ultrasound which reveals this image.
It can be difficult in critical care settings to determine the etiology of worsening respiratory status. In the right clinical context, lung ultrasound can provide useful information that can change management. The society of critical care medicine recommend in their guidelines on page 2485 that ultrasound may be used as a primary diagnostic modality for the ICU patient with respiratory failure. This was a case that I had while on call for CCU a few months ago, and the lung ultrasound images confirmed my clinical suspicion and helped me make my management decision. Although this isn't the ultrasound image from that patient, this image does provide the same ultrasound finding.
That finding is a B-line, or "comet tail sign" which has seven distinct features on lung ultrasound:
Comet tail artifact
Arises from the pleural line
Moves with lung sliding
Hyperechoic
Long without fading
Erases A-lines
Well defined (laser-ray like)
These seven features help to distinguish B-lines from other comet-tail artifacts. Three or more comet tails with these features seen between two ribs in an anterior or lateral ultrasound confirms the presence of an interstitial syndrome. Given her history of recent cardiac arrest and subsequent fluid bolus, the diagnosis of pulmonary edema is likely, which would require diuretic therapy. After giving a dose of intravenous Lasix to this patient, her oxygenation, blood pressure and urine output all improved.
A quick explanation of B-lines by Dr. Daniel Lichtenstein with some notes (including the seven features above) can be seen on video DL-11 at the Hands on Echo Website.
The Toronto General Hospital Department of Anesthesia has a point of care lung ultrasound module on their website. Unfortunately, their is no App version of this module.
This module allows you to view lung ultrasound images from 6 different views with the linear, convex and cardiac probes. Much like their cardiac ultrasound module, the lung reconstruction in the top left corner helps you to relate the images obtained with the probe positioning and anatomy. There is also information on the different structures visualized, commonly seen artifacts, and the assessment possibilities of the different views.
This module provides a general overview on lung ultrasound including how to obtain various lung ultrasound images and how to identify certain structures. This module, however, does not contain any ultrasound images related to pathological findings.
Overall, this is a great module for anyone new to lung ultrasound or for those who wish to review the normal structures as well as the common ultrasound views.
Although radial artery catheter insertion can be done as a palpation-guided procedure, it can sometimes be difficult to perform successfully. This video provides a general overview on how to perform this procedure with ultrasound guidance.
When performing this procedure, the radial artery appears as an anechoic circle that is pulsatile. Unlike the surrounding veins, the radial artery should not be compressible. If you are having difficulty finding the radial artery, the use of colour doppler can help with localization.
A 56 year old gentleman presents to the emergency department with a 2 hour history of crushing central chest pain.
On physical exam, blood pressure is 90/55 with a pulse of 90. Oxygen saturations are 98% on 2 litres nasal prongs. JVP is elevated and there is peripheral edema. Heart sounds are normal with no murmurs appreciated. Lungs are clear on auscultation.
You review the initial ECG:
You perform a quick bedside cardiac ultrasound, and the subcostal view reveals the following image:
This is an example of an inferior myocardial infarction with RV involvement. The physical exam demonstrating predominately symptoms of right-sided heart failure in combination with an ECG with ST elevation in inferior leads would suggest RV involvement.
The bedside cardiac ultrasound can help in confirming RV dysfunction, which is present in the ultrasound image above. The RV sits inferiorly and anteriorly, therefore in the subcostal view it appears closest to the probe at the top of the screen. As you can see, it is not contracting well during systole which confirms the suspected RV involvement.
It is important to consider RV involvement in patients with an inferior STEMI since these patients are usually preload dependent. This modifies how they are treated, and they more often require intravenous fluids to increase their pre-load as well as the avoidance of medications that cause vasodilation (ie: nitrates). Since the presence of RV involvement changes how these patients are managed, bedside cardiac ultrasound can assist with management.
The Toronto General Hospital Department of Anesthesia has an app for Cardiac Ultrasound. Their FOCUS (FOcused Cardiac UltraSound) app is also available to download in the App Store.
This app has several different features. Firstly, it gives a great overview on the different ultrasound views of the heart, including how to obtain these views, how to optimize these views and which structures are assessable with each view. Another great feature of this app is that is provides a great overview of the anatomy with the use of educational diagrams with key anatomical structures labelled. The images and diagrams are clear and easy to read.
The FOCUS app also provides an overview and examples of normal and abnormal pericardium, left ventricular funciton, right ventricular function, and volume status.
This is a great user-friendly and interactive app for anyone who is just starting to learn how to perform bedside cardiac ultrasound, as well as anyone who needs a quick reminder on the essential points.
This video provides an overview of how to use an ultrasound to perform a pericardiocentesis using the cardiac probe.
As with most ultrasound guided procedures, it's important to visualize the needle on insertion and correctly identify the surrounding anatomy. The video provides a good overview of cardiac anatomy as well as the location of a pericardial effusion on echo.
A 43 year old gentleman presents to the emergency department via ambulance with significant shortness of breath.
On clinical exam, he is in respiratory distress, and his blood pressure is 80/40 with a heart rate of 114. The JVP is quite elevated on exam, and there is significant pedal edema. Heart sounds are difficult to appreciate on auscultation, and there are crackles bilaterally on lung auscultation.
You perform a quick bedside ultrasound which reveals the following images:
These images represent a significant pericardial effusion causing cardiac tamponade. Although tamponade is a clinical diagnosis, bedside ultrasonography can aid in the diagnosis (Grade 1C recommendation, Society of Critical Care Medicine 2016).
In these images, both the presence of a significant pericardial effusion as well as right ventricular collapse in diastole support the diagnosis of cardiac tamponade.
The second part of the Society of Critical Care Medicine's guidelines regarding bedside ultrasonography have recently been posted on their website. This part of the guidelines, by Levitov et al., focuses on cardiac bedside ultrasonography in the critical care setting.
This guideline lists several class 1 recommendations for the use of bedside cardiac ultrasonography based on the GRADE system, which demonstrates that there is evidence to support the use of beside cardiac ultrasonography in the evaluation of the critically ill patient.
A 63 year old lady with a history COPD arrives to the emergency department via ambulance acutely short of breath.
She is in respiratory distress with accessory muscle use. Her heart rate is 130, her blood pressure is 90/30, her respiratory rate is 35 and her oxygen saturations are 88% on a 100% non rebreather mask.
You listen to her chest, and you hear decreased breath sounds on the left, and absent breath sounds on the right.
You perform a quick bedside ultrasound of both lungs, starting on the left, that reveals the following images:
This is an example of a tension pneumothorax, which requires urgent treatment with needle decompression and chest tube insertion. Bedside ultrasound is a quick diagnostic test to aid in the diagnosis.
The first images are of a normal lung, with pleural sliding seen on 2D images corresponding with respirations. In M-Mode, the seashore sign can be seen, with the appearance of waves in the top half of the image while the bottom half appears like sand.
In a pneumothorax (00:38), however, there is no longer a pleural slide, and there is the more homogenous "barcode sign" in M-Mode.
Although these ultrasound signs can indicate the presence of a pneumothorax, the diagnosis of a tension pneumothorax is based on clinical signs as described above, particularly the respiratory distress and hemodynamic instability.
This video below describes how to use bedside ultrasonography while performing a paracentesis.
With ultrasound, an area with an adequate amount of free fluid can be identified, and the risk of perforating bowel can be decreased. With the use of the abdominal probe, this area can be identified quickly by scanning the abdomen to obtain both transverse and long axis views.
A 47 year old gentleman presents to the emergency department with fevers, shortness of breath and productive cough. He is tachycardic and is requiring supplemental oxygen. You hear crackles and decreased breath sounds at the base of the right lung.
You perform a bedside lung ultrasound which reveals the following image:
This is an example of a loculated pleural fluid which can be detected on ultrasound. These loculations occur in complicated parapneumonic effusions and empyema. Utrasonography plays a key role in both the diagnoses and management of these effusions. Identifying loculations on ultrasound changes management, since a thoracentesis is required in this circumstance. Also, ultrasound-guided thoracentesis allows you to identify a pocket of fluid that is attainable for sampling.
This resource at Handsonecho by Prof Dr. Daniel Lichtenstein is a great educational resource for lung ultrasound. Included in these short educational videos is the BLUE protocol for acute respiratory failure.
Ultrasound is very useful when performing thoracentesis for both confirming the presence of a pleural effusion and for locating the appropriate area for needle insertion.
This video provides an explanation on ultrasound positioning and landmarking for ultrasound guided thoracentesis.
A 65 year old gentleman presents to the emergency department complaining of sudden sharp chest pain, shortness of breath and lightheadedness.
His pulse is 110, his blood pressure his 90/50, and his oxygen saturations are 92% on 40% venturi mask. His JVP is elevated, but his physical exam is otherwise unremarkable.
You perform a bedside echo which reveals the following image:
This is an example of a pulmonary embolus (PE) leading to hemodynamic instability. Ultrasound has a role when the diagnosis of PE is suspected and the patient is too unstable to undergo a CT or V/Q scan.
The ultrasound image above is an apical view of the heart, with the ventricles at the top of the image and the right side of the heart on the left side of the screen. As you can see, the right ventricle (RV) is enlarged, and is larger than the left ventricle in this image. Also, there is hyperkinesis of the apex of the RV with akinesis of the mid free wall. This distinct pattern of RV dysfunction on ultrasound is typical in cases of PE and is known as McConnell's sign.
One of the procedures where ultrasound is useful is for central line insertion into the jugular vein. In fact, ultrasound guidance for internal jugular line placement is considered standard of care.
The ultrasound portion of the technique begins at 3:43. You can use the transverse (at 5:00) or longitudinal view (at 5:05) to visualize the tip of the needle as it is inserted into the jugular vein.
When inserting the needle, you should assure the following:
- The internal jugular is centered on the ultrasound image
- The ultrasound probe is perpendicular to the needle's insertion angle is using the transverse view
- The needle's insertion point is at the middle of the ultrasound probe
As mentioned in the video, you should also confirm that the wire is correctly positioned in the jugular vein before proceeding with dilating.
Ultrasound Podcast is a great resource with podcasts that discuss the applications of bedside ultrasound. Their podcasts include recent trials as well as plenty of cases and ultrasound images.
A 45-year-old lady presents to the emergency department after experiencing chest pain at her mother's funeral. An ECG performed reveals ST segment elevation in the V1-V4 leads. She undergoes emergency cardiac catheterization, but coronary arteries are normal.
A bedside echocardiogram performed after the procedure reveals the following images:
This case is an example of Takotsubo Cardiomyopathy, or "broken heart syndrome". It is an acute presentation of left ventricular systolic dysfunction that is very similar to myocardial infarction. Howeverm the dysfunction in Takotsubo Cardiomyopathy is not confined to one artery territory, nor is there any occlusive coronary artery disease found on cardiac catherterisation.
Generally, the systolic dysfunction affects the mid-apical portions of the left ventricle, causing the classic "apical ballooning pattern" as seen in the video above. The term "Takotsubo Cardiomyopathy" comes from this pattern seen on echography, which is similar to the Japanese octopus trap of the same name pictured below.
The first ultrasound image demonstrates the apical ballooning of the left ventricle. The second view demonstrates the difference in contractility of the apical and mid regions compared to the basal regions of the heart. As you can see, there is better contraction of the left ventricle in later images, which corresponds with the more basal regions of the heart.
Takotsubo Cardiomyopathy is a great example of how bedside ultrasound can be used to assist with the diagnosis of certain clinical entities.
Here are two websites with guidelines, resources and modules for ultrasound training.
The first is The American Institute of Ultrasound in Medicine's website, which includes physician training guidelines, official statements, ultrasound parameters as well as an ultrasound curriculum.
The second is the Society of Ultrasound in Medical Education's website. It includes a curriculum database of curricula from several different universities as well as learning modules that range from ultrasound theory to its application.
Both of these websites contain great resources for medical professionals at any level of ultrasound training looking to refine their skills, attend an upcoming ultrasound worksop/conference, teach ultrasound skills to learners, or develop an ultrasound curriculum for their institution.
I had a few opportunities this week to use a handheld ultrasound while on call, and I was quite impressed with the experience. I was able to quickly assess volume status, gross cardiac function and rule out significant pleural effusions quickly and easily on a few of the patients that were admitted.
The handheld ultrasound is built for a busy clinical environment. Its relatively small size allowed for rapid access and use. The device functions were very intuitive, and I found I was able to use the colour functions and adjust the depth and gain easily. Although the screen is small, I found that the images captured were of good quality and aided me in my clinical diagnosis.
Although great for clinical use in urgent care settings, I do not think the handheld ultrasound is ideal for clinical teaching. The larger portable machines have a screen size that is more suitable for teaching small groups. Also, I feel that trainees may need to have a few sessions with larger ultrasound machines before attempting to capture images with a handheld device.
All in all, I was quite impressed with the handheld machine, and I would definitely use one again if it was available.
Part 1 of the Society of Critical Care Medicine Guidelines for Bedside Ultrasonography were published by Frankel et al. in November of 2015. These guidelines include recommendations on several non-cardiac applications of bedside ultrasonography in critically ill patients. In particular, there were strong recommendations for the use of ultrasound in procedures such as thoracentesis, paracentesis and central line insertion.
The written guidelines can be found here. There is also an iCritical Care Podcast by Dr. Ludwig Lin and Dr. Michael Blavais that comments on these guidelines, discusses the integration of technology into ultrasound application and practice, and provides suggestions for ultrasound training of learners and practicing physicians.
Part 2 of these guidelines, which includes the cardiac applications of bedside ultrasonography, have recently been published, and I will post the link once they are up on the Society of Critical Care Medicine's website.
The Dalhousie Internal Medicine Residents are running in this year's Bluenose Marathon to fundraise for a new ultrasound machine for the Medical Teaching Unit at the Halifax Infirmary.
Information on their fundraising campaign can be found here.
Point of care ultrasound (POCUS) is an emerging tool used at the bedside to evaluate patients in emergency departments, hospital departments, and intensive care units. The use of ultrasound guidance for certain clinical procedures has become the standard of care. This technology has the potential to aid in the diagnosis and management of patients as well as increase patient safety during bedside procedures.
This blog will serve as a resource for information on bedside ultrasound and its various applications. These resources will include society guidelines, review articles, clinical trials and published educational interventions. These resources will inform my reflections on how beside ultrasound has impacted clinical care, medical practice and medical education.