A 62 year old gentleman is 6 days post cardiac bypass surgery. The ICU has had difficulty weaning the patient from the ventilator.
Over the past 24 hours, the patient's ventilator requirements have increased. There have also been an increase in endotracheal secretions.
You perform a bedside ultrasound, which reveals this image:
This is an example of consolidation seen on ultrasound secondary to a ventilator-associated pneumonia. Non-translobar consolidation is confirmed by the "shred sign", which is seen as the irregular line at the bottom of the screen. This irregular line marks the boundary between the consolidated and non-consolidated lung.
It is important to differentiate atelectasis from pneumonia when consolidation is present on ultrasound. The dynamic air bronchograms, as seen above, are more suggestive of a pneumonia. In the image above, clear, anechoic airways are visualized, and these airways change dynamically during inspiration and expiration.
For more information on signs of consolidation and dynamic air bronchograms, check out Dr. Lichtenstein's videos below.
This app provides information on interpretation of ultrasound images in 6 systems:
In each system, a labelled image with normal values for ultrasonography interpretation is presented. See the aortic root example below:
This App provides a quick reference to look up the relative position of structures in various ultrasound views as well as the normal reference ranges for these structures. However, this App does not provide information on probe positioning or on capturing these images. This App serves as a good resource for quick identification and interpretation of various structures in the systems listed above.
Another good feature of this App is the "Links" Section on the home page, which provides links to Emergency and Intensive Care Ultrasound resources, online lectures, image archives and core articles. Some of the links don't work, but most of them do work and provide great background information on point of care ultrasound.
Overall, this App serves both as a quick reference guide for point-of-care ultrasound interpretation as well as a source of information for those with background knowledge in point-of-care ultrasound.
These two videos demonstrate the ultrasound techniques for femoral artery and vein catheter insertions.
First, the femoral artery catheter insertion:
Second, the femoral vein catheter insertion:
These are both very similar, since you will be locating both the femoral artery and vein when you perform either procedure.
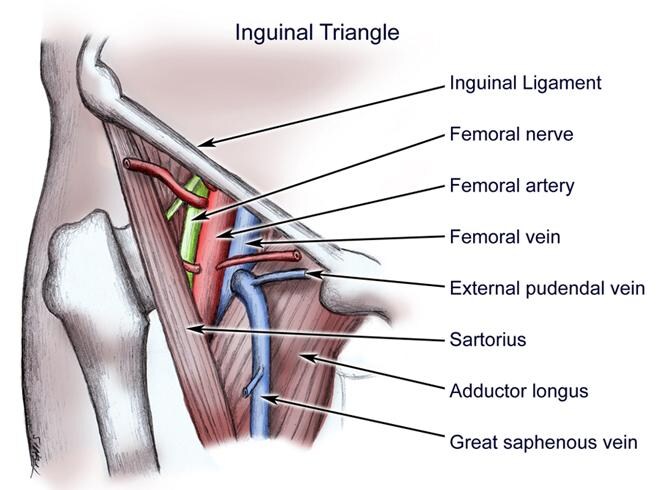
Localization of both of these structures is key when performing these procedures. It is important to remember the anatomy of the femoral region. The femoral artery runs laterally to the femoral vein and medially to the femoral nerve as in the figure below.
However, anatomical variants do exist, so this is not always the case. To further help with localization of your chosen vessel, remember that that veins are compressible on ultrasound, while arteries are not.
A 63-year old lady was admitted to the coronary care unit post cardiac arrest with return of spontaneous circulation. She was intubated for a decreased level of consciousness following resuscitation and was placed on a hypothermia protocol. You are called to assess her for low blood pressure and increasing oxygen requirements.
On exam, her blood pressure is 100/60 with a pulse of 90. Temperature is at target for the hypothermia protocol. Oxygen saturations are 90% with an Fi02 of 0.8 and a PEEP of 10 cm H20. Her JVP is difficult to appreciate. Heart sounds are rapid, with no additional heart sounds or murmurs appreciated on initial assessment. There are crackles on lung auscultation.
You quickly review the chart, and noticed that this patient was given a 500 mL bolus earlier this afternoon for hypotension and decreased urine output. Her urine output has been minimal (30 mL total) since the bolus 4 hours ago. Also, the PEEP has been increased from 8 to 10 cm H20, and the Fi02 was progressively increased from 0.6 to 0.8.
You've ordered an initial chest X-ray, ECG and bloodwork. While waiting for these tests to be performed, you perform a quick bedside lung ultrasound which reveals this image.
It can be difficult in critical care settings to determine the etiology of worsening respiratory status. In the right clinical context, lung ultrasound can provide useful information that can change management. The society of critical care medicine recommend in their guidelines on page 2485 that ultrasound may be used as a primary diagnostic modality for the ICU patient with respiratory failure. This was a case that I had while on call for CCU a few months ago, and the lung ultrasound images confirmed my clinical suspicion and helped me make my management decision. Although this isn't the ultrasound image from that patient, this image does provide the same ultrasound finding.
That finding is a B-line, or "comet tail sign" which has seven distinct features on lung ultrasound:
Comet tail artifact
Arises from the pleural line
Moves with lung sliding
Hyperechoic
Long without fading
Erases A-lines
Well defined (laser-ray like)
These seven features help to distinguish B-lines from other comet-tail artifacts. Three or more comet tails with these features seen between two ribs in an anterior or lateral ultrasound confirms the presence of an interstitial syndrome. Given her history of recent cardiac arrest and subsequent fluid bolus, the diagnosis of pulmonary edema is likely, which would require diuretic therapy. After giving a dose of intravenous Lasix to this patient, her oxygenation, blood pressure and urine output all improved.
A quick explanation of B-lines by Dr. Daniel Lichtenstein with some notes (including the seven features above) can be seen on video DL-11 at the Hands on Echo Website.
The Toronto General Hospital Department of Anesthesia has a point of care lung ultrasound module on their website. Unfortunately, their is no App version of this module.
This module allows you to view lung ultrasound images from 6 different views with the linear, convex and cardiac probes. Much like their cardiac ultrasound module, the lung reconstruction in the top left corner helps you to relate the images obtained with the probe positioning and anatomy. There is also information on the different structures visualized, commonly seen artifacts, and the assessment possibilities of the different views.
This module provides a general overview on lung ultrasound including how to obtain various lung ultrasound images and how to identify certain structures. This module, however, does not contain any ultrasound images related to pathological findings.
Overall, this is a great module for anyone new to lung ultrasound or for those who wish to review the normal structures as well as the common ultrasound views.
Although radial artery catheter insertion can be done as a palpation-guided procedure, it can sometimes be difficult to perform successfully. This video provides a general overview on how to perform this procedure with ultrasound guidance.
When performing this procedure, the radial artery appears as an anechoic circle that is pulsatile. Unlike the surrounding veins, the radial artery should not be compressible. If you are having difficulty finding the radial artery, the use of colour doppler can help with localization.
A 56 year old gentleman presents to the emergency department with a 2 hour history of crushing central chest pain.
On physical exam, blood pressure is 90/55 with a pulse of 90. Oxygen saturations are 98% on 2 litres nasal prongs. JVP is elevated and there is peripheral edema. Heart sounds are normal with no murmurs appreciated. Lungs are clear on auscultation.
You review the initial ECG:
You perform a quick bedside cardiac ultrasound, and the subcostal view reveals the following image:
This is an example of an inferior myocardial infarction with RV involvement. The physical exam demonstrating predominately symptoms of right-sided heart failure in combination with an ECG with ST elevation in inferior leads would suggest RV involvement.
The bedside cardiac ultrasound can help in confirming RV dysfunction, which is present in the ultrasound image above. The RV sits inferiorly and anteriorly, therefore in the subcostal view it appears closest to the probe at the top of the screen. As you can see, it is not contracting well during systole which confirms the suspected RV involvement.
It is important to consider RV involvement in patients with an inferior STEMI since these patients are usually preload dependent. This modifies how they are treated, and they more often require intravenous fluids to increase their pre-load as well as the avoidance of medications that cause vasodilation (ie: nitrates). Since the presence of RV involvement changes how these patients are managed, bedside cardiac ultrasound can assist with management.